Full HTML
Air in the water: A case of emphysematous cystitis and point-of-care ultrasound in the emergency department
O Gómez Maria Alejandra1, O Cardozo Alejandro2, P García Manuel Alejandro2
Author Affiliation
1General physician, Department of Emergency, Fundación Instituto Neurológico de Colombia, Medellín, Colombia,
2Emergency Physician, Department of Emergency, Fundación Instituto Neurológico de Colombia, Medellín, Colombia
Abstract
Emphysematous cystitis is a rare and potentially fatal complication of urinary tract infections. We present a case of bacterial emphysematous cystitis in a 59-year-old woman who presented with behavioral changes, aggression, visual hallucinations, unintentional weight loss, fecal incontinence, and occasional diarrhea for two months. The diagnosis was suspected by abdominal ultrasound and confirmed by abdominal computed tomography. This highlights the importance of imaging as a diagnostic tool for emphysematous cystitis, particularly point-of-care ultrasound in the emergency department, due to its sensitivity and freedom from radiation.
DOI: 10.32677/yjm.v2i3.4290
Pages: 177-178
View: 6
Download: 12
DOI URL: https://doi.org/10.32677/yjm.v2i3.4290
Publish Date: 19-12-2023
Full Text
Introduction
Emphysematous cystitis is a rare and potentially life-threatening complication of urinary tract infections characterized by the presence of air in the lumen or wall of the bladder. Women, older people, diabetics, and immunocompromised people are particularly affected [1]. It is caused by microorganisms that can ferment glucose or proteins in urine. The clinical features are non-specific and the diagnosis can be particularly difficult without the aid of imaging studies. A point-of-care ultrasound scan can be used to assess the bladder. If artifacts are found that suggest air in the bladder, emphysematous cystitis is suspected. Treatment of this complication is based on targeted antibiotic therapy and bladder emptying. Early administration of antibiotics can prevent complications such as hydronephrosis, emphysematous pyelonephritis, sepsis, necrosis, and bladder rupture [2]. In this report, we present a patient who visited our department and whose initial bedside ultrasound examination alerted us to the suspicion of emphysematous cystitis as the cause of his symptoms..
CASE REPORT
A 59-year-old woman with a history of non-insulin-dependent diabetes mellitus presented with a two-month history of behavioral changes, aggression, visual hallucinations, unintentional weight loss, fecal incontinence, and occasional diarrhea. On admission, she was conscious but disoriented and complained of diffuse abdominal tenderness without peritoneal irritation. Initial laboratory tests revealed mild hyponatremia and mild hyperkalemia. Urinalysis showed pyuria, hematuria, bacteriuria, glucosuria, and positive nitrites.
Initial ultrasound examination revealed a thickened bladder wall and hyperechoic punctate images with reverberation artifacts, suggesting the presence of air in the suprapubic window (Figures 1A and 1B). Subsequent imaging studies, including head computed tomography, which excluded structural intracerebral lesions, and contrast-enhanced computed tomography of the abdomen and pelvis, revealed irregular and diffuse bladder wall thickening associated with intramural and endoluminal air (Figure 2), consistent with a diagnosis of emphysematous Cystitis.
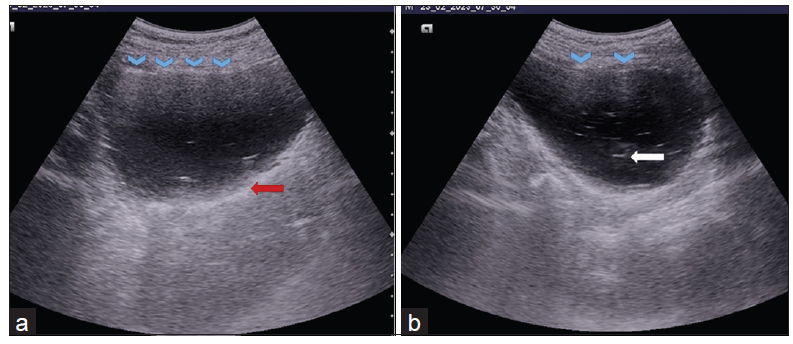
Figure 1: (a and b) Reverberation (blue head arrows), hyperechoic ring (red arrow), and comet tail (white arrow)
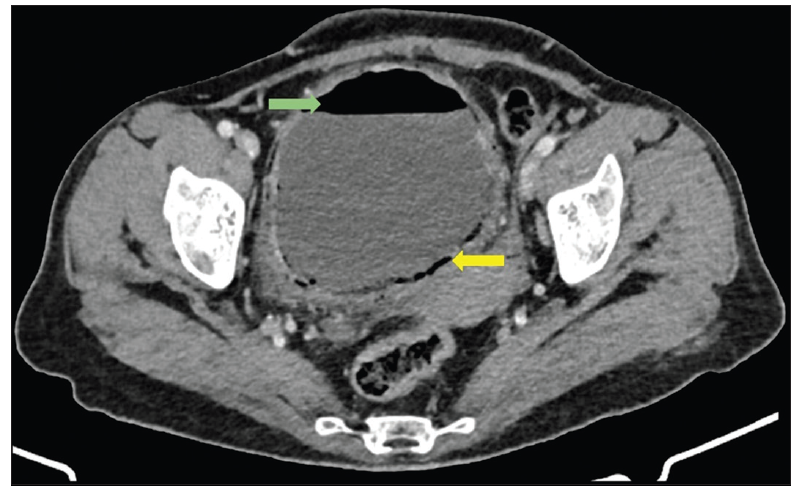
Figure 2: Gas in the bladder (green arrow) and gas in the wall (yellow arrow). Finding of computed tomography of the abdomen and pelvis in emphysematous cystitis
The patient was hospitalized and received empirical antibiotic therapy while urine culture results were pending. In the following days, ampicillin-resistant Escherichia coli was detected in urine culture as the causative agent of emphysematous cystitis, and targeted intravenous antibiotic therapy, strict blood sugar control and bladder drainage were initiated, which led to a good result.
DISCUSSION
Emphysematous cystitis is an uncommon necrotizing infection with high morbidity and mortality, characterized by the accumulation of gas in the bladder lumen and wall. The most significant risk factors include diabetes mellitus (up to 80%), bladder outlet obstruction, recurrent urinary tract infections, neurogenic bladder, immunosuppression, female gender and organ transplantation [3]. The most commonly isolated pathogens are bacteria, especially Escherichia coli (70-75%), which have the property of producing gas and generating carbon dioxide by fermenting the high concentrations of glucose in the urine and tissues of affected patients. By accumulating acid radicals that lower the local pH, the bacteria themselves, which have specific enzymes, can convert the acids into carbon dioxide [4].
Emphysematous cystitis has no specific signs or symptoms and requires radiological studies to confirm the diagnosis. The presentation can vary from asymptomatic to severe sepsis. More than half of patients suffer from abdominal pain, classic symptoms of acute cystitis and pneumaturia. Although pneumaturia appears to be a very specific symptom, it is a rare patient complaint [5]. A plain abdominal radiograph has high sensitivity (97%) and can reveal gas as an air density line that delimits the bladder circumference. Ultrasound detection of a hyperechoic ring could be considered pathognomonic for emphysematous cystitis [2]. However, the interpretation of the possibility of intravesical air is based on familiarity with artifacts that are frequently labeled as pathological. In our case, we encountered an ultrasonic artifact called reverberation, which occurs when an ultrasonic wave hits two powerful reflectors and bounces between them, creating a pattern of repeated parallel lines separated by the same distance. This goes against the notion that following a reflection, an echo would come back to the transducer. In our case, the visible artifact lies between the original structure (bladder) and the second reflector, which is air in emphysematous cystitis [6]. If the reflector is small, such as gas bubbles, cholesterol crystals in the bladder wall, or metallic materials such as clamps, pellets, and projectiles, the artifact resembles a "comet tail," which is considered a form or subtype of reverberation (Figure 1B), similar to the " B lines” that are seen in an interstitial pattern on the lung surface [7].
Finally, computed tomography of the abdomen is the most sensitive and specific diagnostic tool that confirms the diagnosis and allows accurate assessment of the location, distribution of intramural air, and detection of intravesical air-fluid levels [4].
Conclusion
The timely diagnosis of complications of urinary tract infections, such as: B. emphysematous cystitis, is essential for appropriate treatment and better chances of success. Interpretation of artifacts suggestive of air in water using bedside ultrasound raises suspicion of an additional diagnosis not suggested by physical examination. This reinforces the utility of point-of-care ultrasound in the emergency department, not only in the evaluation of renal colic but also in complicated urinary tract infections, such as emphysematous cystitis..
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and all accompanying images
AUTHORS’ CONTRIBUTIONS
All authors contributed to the completion of this work. The final manuscript was read and approved by all author
References
- Igúzquiza Pellejero MJ, Torres Courchoud I, Navarro Aguilar ME. Emphysematous cistitis. Rev Clin Esp. 2020 Feb 11:S0014- 2565(19)30303-0.
- Tanabe A, Fujita Y, Amagai T. A hyperechoic bladder-ring appearance as pathognomonic finding for emphysematous cystitis – A case report and literature review. Radiol Case Rep. 2021;16(9):2457-2459.
- Young YR, Sheu BF, Lee CC, et al. Images in Emergency Medicine. Ann Emerg Med. 2008;51(3):230-261
- Moreno Caballero L, Navas Campo R, Ibáñez Muñoz D. Emphysematous cystitis. Med Clin (Barc). 2021 Sep 24;157(6):311.
- Amano M, Shimizu T. Emphysematous cystitis: a review of the literature. Intern Med. 2014;53(2):79–82.
- Quien MM, Saric M. Ultrasound imaging artifacts: How to recognize them and how to avoid them. Echocardiography. 2018;35(9):1388-1401.
- Bönhof J. Ultrasound Artifacts – Part 1. Ultraschall Med Eur J Ultrasound. 2015;37(02):140-156.